Undergoing in vitro fertilization (IVF) represents a significant emotional, physical, and financial investment. When a chemical pregnancy after IVF occurs, the disappointment can feel particularly acute. Understanding why biochemical pregnancy happens in fertility treatment, how common it is, and what can be done to improve outcomes is essential for anyone navigating the IVF journey.
What Is a Chemical Pregnancy After IVF?
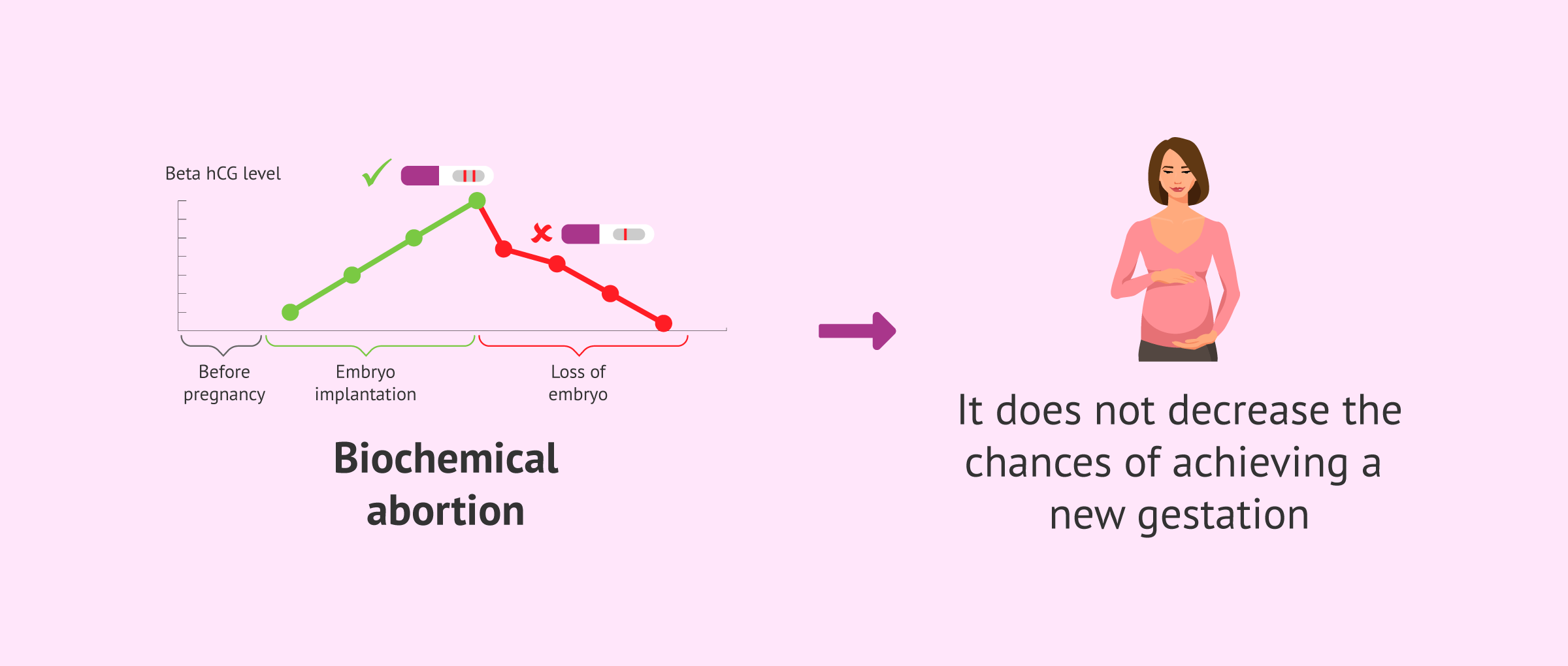
A chemical pregnancy after IVF is defined identically to a spontaneous chemical pregnancy: a positive pregnancy test (detecting hCG) followed by declining hormone levels before a gestational sac can be visualized on ultrasound. In IVF cycles, this is typically detected through beta hCG blood tests performed approximately 10-14 days after embryo transfer.
In fertility treatment, chemical pregnancies are sometimes called “biochemical pregnancies” or “biochemical losses.” The terminology is interchangeable, though fertility clinics may prefer “biochemical” in clinical documentation.
How Common Is Chemical Pregnancy After IVF?
Chemical pregnancy rates in IVF are surprisingly high and represent a significant portion of treatment failures. Research indicates:
- 18-22% of IVF pregnancies end as biochemical pregnancies
- Up to 33% of positive hCG results after frozen embryo transfer result in biochemical loss
- The rate increases with maternal age, particularly after age 38
- Single top-quality embryo transfers in women under 38 still result in biochemical pregnancy approximately 8% of the time
These statistics can feel discouraging, but they also reflect the reality that IVF overcomes many barriers to conception while still being subject to the biological challenges of early embryo development.
Why IVF Doesn’t Prevent Chemical Pregnancy
IVF addresses many fertility challenges—blocked tubes, low sperm count, anovulation—but it cannot control the fundamental biology of early embryo development. The primary causes of chemical pregnancy after IVF mirror those in natural conception:
Embryo Chromosomal Abnormalities Even with high-quality embryos selected for transfer, chromosomal abnormalities remain the leading cause of biochemical loss. PGT-A (preimplantation genetic testing) can identify aneuploid embryos before transfer, but it is not 100% accurate, and some mosaic embryos may test normal while still carrying abnormalities.
Uterine Receptivity Issues IVF cannot force a uterus to be receptive. The window of implantation is narrow—typically 24-48 hours—and if the embryo and uterine lining are not perfectly synchronized, implantation fails or is incomplete. Factors affecting receptivity include:
- Endometrial thickness under 9mm at transfer
- Endometrial pattern (a trilaminar pattern is ideal)
- Uterine blood flow
- Endometrial microbiome balance
Hormonal Support Gaps IVF cycles rely on external hormone support rather than the body’s natural production. Inadequate progesterone or estrogen supplementation can lead to luteal phase support failure, causing the uterine lining to shed despite initial implantation.
Ovarian Stimulation Effects The medications used to stimulate egg production may affect egg quality or the endometrial environment. Some research suggests that high stimulation protocols can create a slightly less receptive uterine lining compared to natural cycles.
The IVF Chemical Pregnancy Timeline
Day 0: Embryo transfer Days 1-3: Embryo hatches from its shell and begins contacting the uterine lining Days 4-6: Implantation begins; trophoblast cells start producing hCG Day 10-14: First beta hCG blood test Days 14-21: Second beta hCG test to assess doubling Days 21-28: If hCG declines or fails to rise appropriately, biochemical pregnancy is diagnosed Week 5-6: Ultrasound would normally show gestational sac; in biochemical pregnancy, nothing is visible
The compressed timeline of IVF monitoring means biochemical pregnancies are detected more consistently than in natural conception, where many women never test before a missed period.
Diagnosis in IVF Cycles
IVF clinics diagnose biochemical pregnancy through:
Serial Beta hCG Testing:
- First test 10-14 days after transfer
- Second test 48 hours later
- In viable pregnancies, hCG should increase by at least 66% every 48 hours
- Stagnant or declining levels indicate biochemical loss
Ultrasound Confirmation:
- If hCG levels are borderline, a transvaginal ultrasound at 5-6 weeks confirms whether a gestational sac is present
- No visible sac with hCG above 1,500-2,000 mIU/mL suggests ectopic pregnancy or biochemical loss
Emotional Impact After IVF
A chemical pregnancy after IVF carries unique emotional weight. You’ve invested months in preparation, endured injections and procedures, paid significant costs, and carried immense hope. A biochemical loss can feel like cruel teasing—a positive test that vanishes before it becomes “real.”
Many patients report that biochemical pregnancies are harder to process than negative cycles because there was momentary hope. The grief is complicated by financial concerns, pressure about remaining embryos, and decisions about future treatment.
Prevention Strategies in Future IVF Cycles
Preimplantation Genetic Testing (PGT-A) Testing embryos for chromosomal normality before transfer significantly reduces biochemical pregnancy rates. PGT-A identifies aneuploid embryos that would likely fail to develop, allowing transfer of only chromosomally normal embryos.
Endometrial Receptivity Analysis (ERA) This specialized test evaluates the optimal timing for embryo transfer based on gene expression in the endometrial lining. For women with recurrent implantation failure or biochemical pregnancy, ERA can identify a displaced window of implantation, allowing precisely timed “personalized” transfers.
Improved Luteal Phase Support
- Higher dose progesterone supplementation
- Addition of estrogen in some protocols
- Extended progesterone support through 10-12 weeks in some cases
- Intramuscular progesterone injections rather than vaginal suppositories for better absorption
Endometrial Scratching A minor procedure that intentionally creates a small injury to the endometrium may trigger a healing response that improves receptivity. Research results are mixed, but some studies show benefit for recurrent implantation failure.
Immune Testing and Treatment For women with recurrent biochemical pregnancy after IVF, immune testing may reveal:
- Elevated natural killer cells
- Antiphospholipid antibodies
- Thrombophilias
- HLA compatibility issues between partners
Targeted treatments include intralipid infusions, steroids, anticoagulants, and IVIG.
Lifestyle Optimization Between Cycles
- CoQ10 supplementation (600 mg daily for 3 months) to improve egg quality
- DHEA for women with diminished ovarian reserve
- Antioxidant-rich diet
- Stress reduction and adequate sleep
- Avoiding environmental toxins
Success Rates After Biochemical Pregnancy IVF
The encouraging news is that a biochemical pregnancy after IVF demonstrates that implantation can occur. Many fertility specialists view this as a positive prognostic sign. With appropriate adjustments to protocol, success rates in subsequent cycles are often excellent.
Studies show that women who experience biochemical pregnancy in an IVF cycle have similar or slightly better cumulative success rates than those with negative cycles, provided underlying issues are addressed.
When to Consider Donor Options
If recurrent biochemical pregnancy after IVF occurs with:
- Multiple PGT-A normal embryos
- Corrected uterine issues
- Optimized hormonal support
- Advanced maternal age (over 42)
Your doctor may discuss donor egg or donor embryo options. These eliminate age-related egg quality issues and often result in significantly higher success rates.
Moving Forward
A chemical pregnancy after IVF is devastating but not the end of your fertility journey. Work closely with your reproductive endocrinologist to analyze what happened and adjust your protocol. Many couples who experience biochemical loss go on to achieve successful pregnancies in subsequent cycles. Your previous cycle provided valuable information that brings you closer to your goal.